The arteriovenous graft has been a workhorse of hemodialysis access for decades. It is reliable, technically straightforward to place, and gives clinicians a predictable conduit for dialysis. It also creates a low-resistance pathway between artery and vein that drives a continuous high-flow circuit through the heart — present around the clock, not only during dialysis sessions. That continuous flow is the variable this platform is designed to address.

What the platform is designed to do
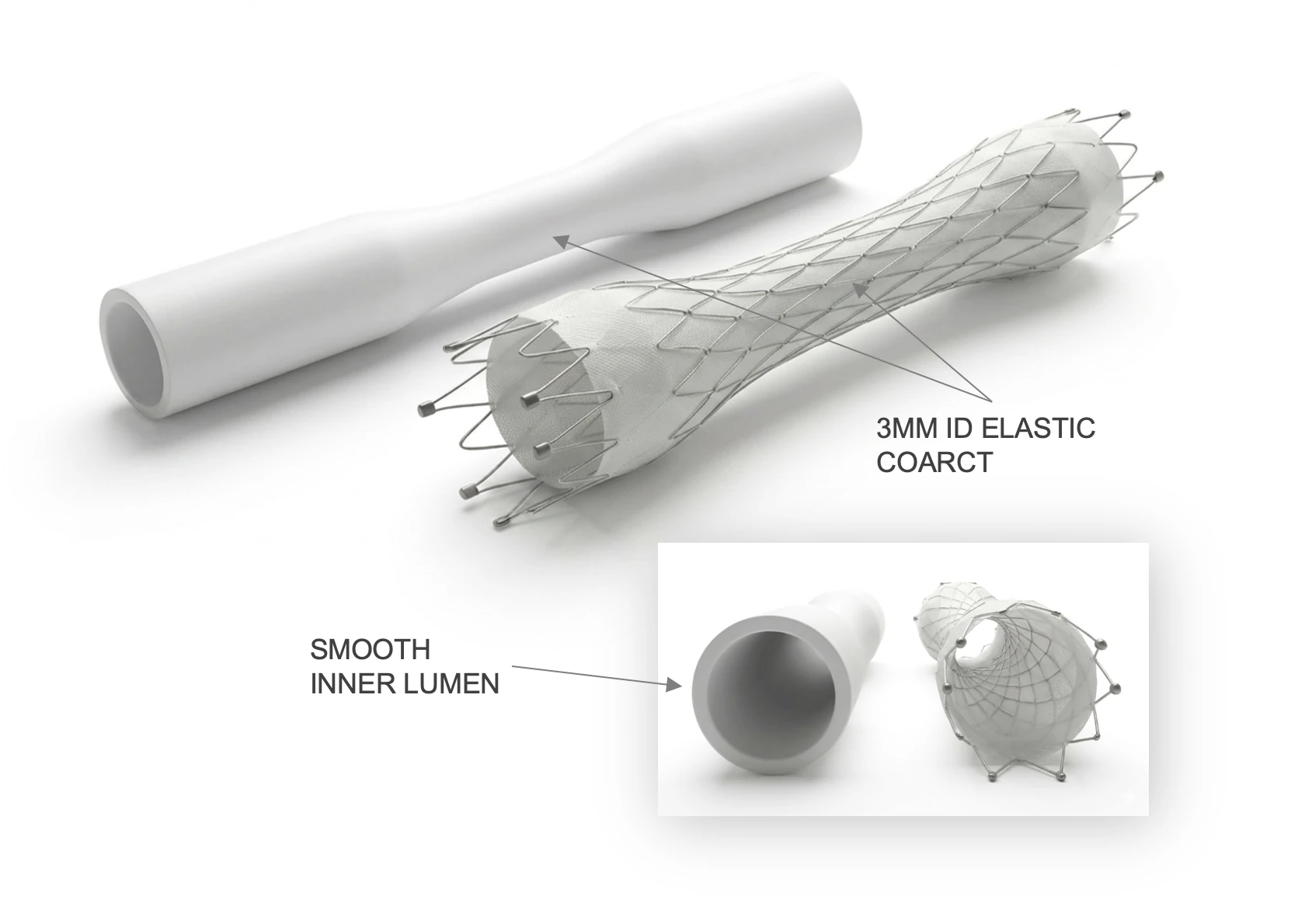
A flow-control AV graft is built around the recognition that the dialysis machine and the heart have different flow needs. The machine draws only a portion of the access flow through the dialyzer during a treatment session; the remainder is continuous extra work for the heart between sessions. The graft is designed to deliver the flow needed during dialysis while limiting that continuous excess, using a calibrated internal geometry intended to limit access flow without occluding the access.
The design intent is to preserve dialysis adequacy during treatment while reducing the continuous between-session burden — a two-sided goal. Whether a given device achieves that goal in practice is an empirical question to be answered by preclinical and clinical evidence.
Elastic flow-control mechanism · developed by VascX
Why access flow matters
End-stage renal disease affects a large and growing population — on the order of 800,000 people in the United States — most of whom depend on hemodialysis and therefore on durable vascular access. AV grafts are an important access option, especially for patients whose veins are not suitable for a fistula.
Like fistulas, AV grafts create a sustained low-resistance circuit between artery and vein, increasing venous return and cardiac output demand continuously. Excessive access flow is associated with cardiac burden in some patients, including cardiac remodeling, pulmonary hypertension, and high-output heart failure in susceptible patients. Reducing excessive access flow without compromising dialysis adequacy is the underlying goal of flow-control AV graft design.
Cannulation and intervention compatibility
An AV graft has to be cannulated for every dialysis treatment and may need standard interventions over its lifespan. Thrombectomy in particular — the procedure used to clear clot and restore access patency — is part of the routine clinical management of grafts. This platform is designed to support standard cannulation patterns and to accept standard interventions, including thrombectomy.
Part of the VascX flow-control platform
The flow-control AV graft is one half of the VascX elastic flow-control platform. Its companion — the flow-control stent — introduces flow control into existing fistulas and grafts, so the platform can address both new access creation and existing high-flow access.

Developed by our subsidiary
The flow-control AV graft is developed by VascX, Principal Medical's dialysis-access subsidiary, as part of its patented elastic flow-control platform. For the full technical detail on the device and platform, visit the VascX site.
Read more at vascx.com →
Investigational status: Principal Medical's portfolio platforms and the products referenced here are currently in development and are not yet cleared or approved by the U.S. Food and Drug Administration.