Lower-extremity bypass is a routine procedure for patients with occluded arteries, restoring blood supply to a limb by routing around the blockage with a graft. But the graft is only as durable as the flow through it. In patients with poor distal arterial outflow — the low-outflow states where the target vessels beyond the graft are themselves diseased — blood moves slowly, and slow flow invites thrombosis and early graft occlusion. For these patients, keeping the graft open is the central challenge.

Refining the distal arteriovenous fistula
One established way to keep flow moving through a struggling bypass is the distal arteriovenous fistula (DAVF) — a connection that adds venous outflow to raise flow and improve patency. DAVF works, but it comes with trade-offs: it is technically difficult to place, and by directing arterial pressure into the leg's veins it tends to cause lower-extremity swelling.
Principal Medical's bypass graft is designed to preserve the flow benefit of DAVF while removing what makes it difficult. It is built like a traditional bypass graft, with one addition: a return limb that connects the distal graft back to a vein near the proximal anastomosis, returning blood into the venous system above the valves. Routing the return flow above the valves is what is intended to eliminate the swelling associated with DAVF.
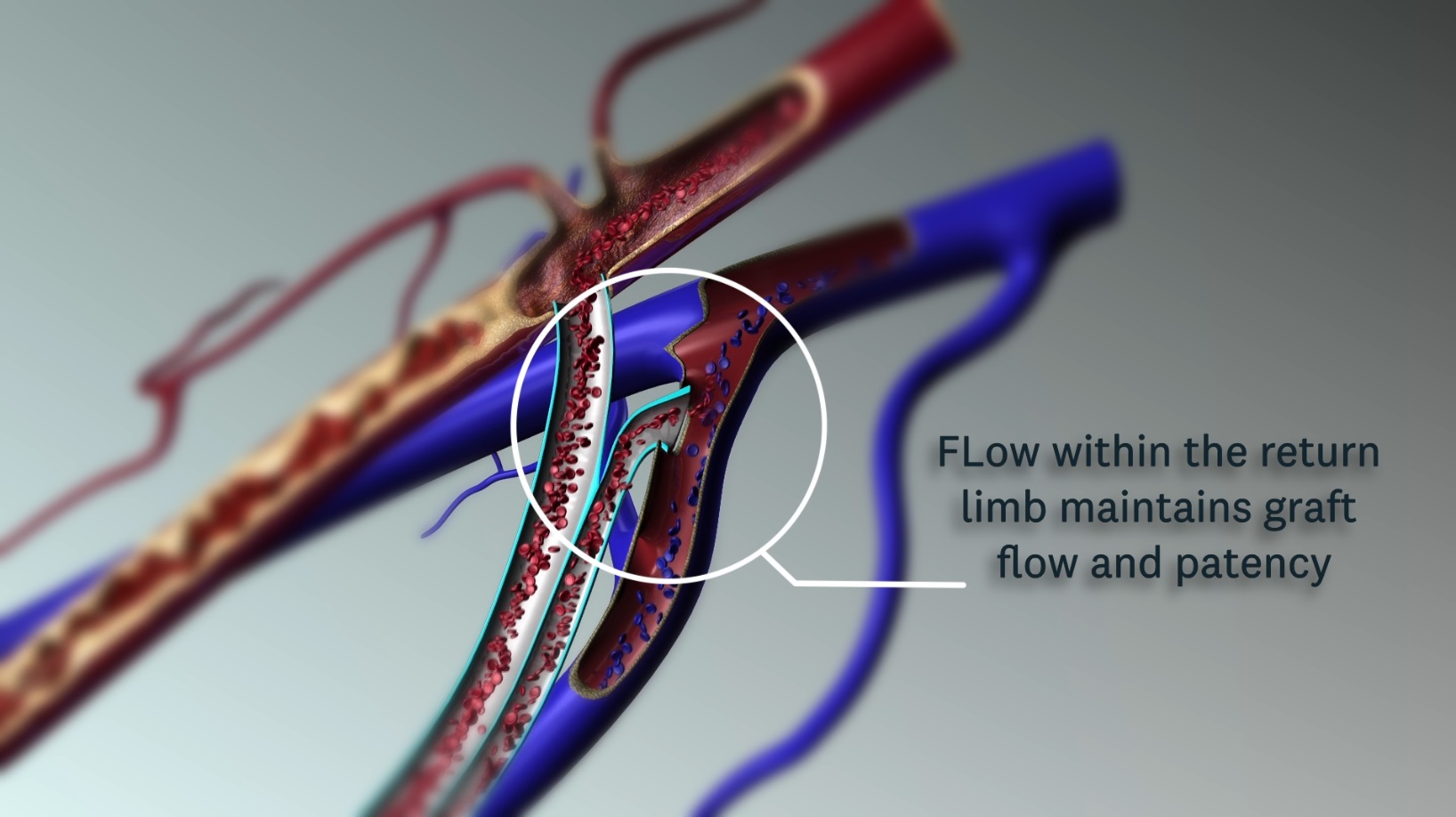
How the return limb works
The return limb is designed to maintain flow through the graft even when the patient's distal arterial outflow is poor — the situation in which a conventional bypass is most likely to fail. Because the added connection is a single anastomosis to the proximal vein, it is intended to fit within the existing procedure: one additional connection, with no additional incisions and no additional healing time beyond the standard bypass.
The graft itself is constructed from expanded polytetrafluoroethylene (ePTFE), the material used in conventional bypass grafts, so the device is intended to behave like a familiar graft to the operating surgeon while adding the return-limb flow path.
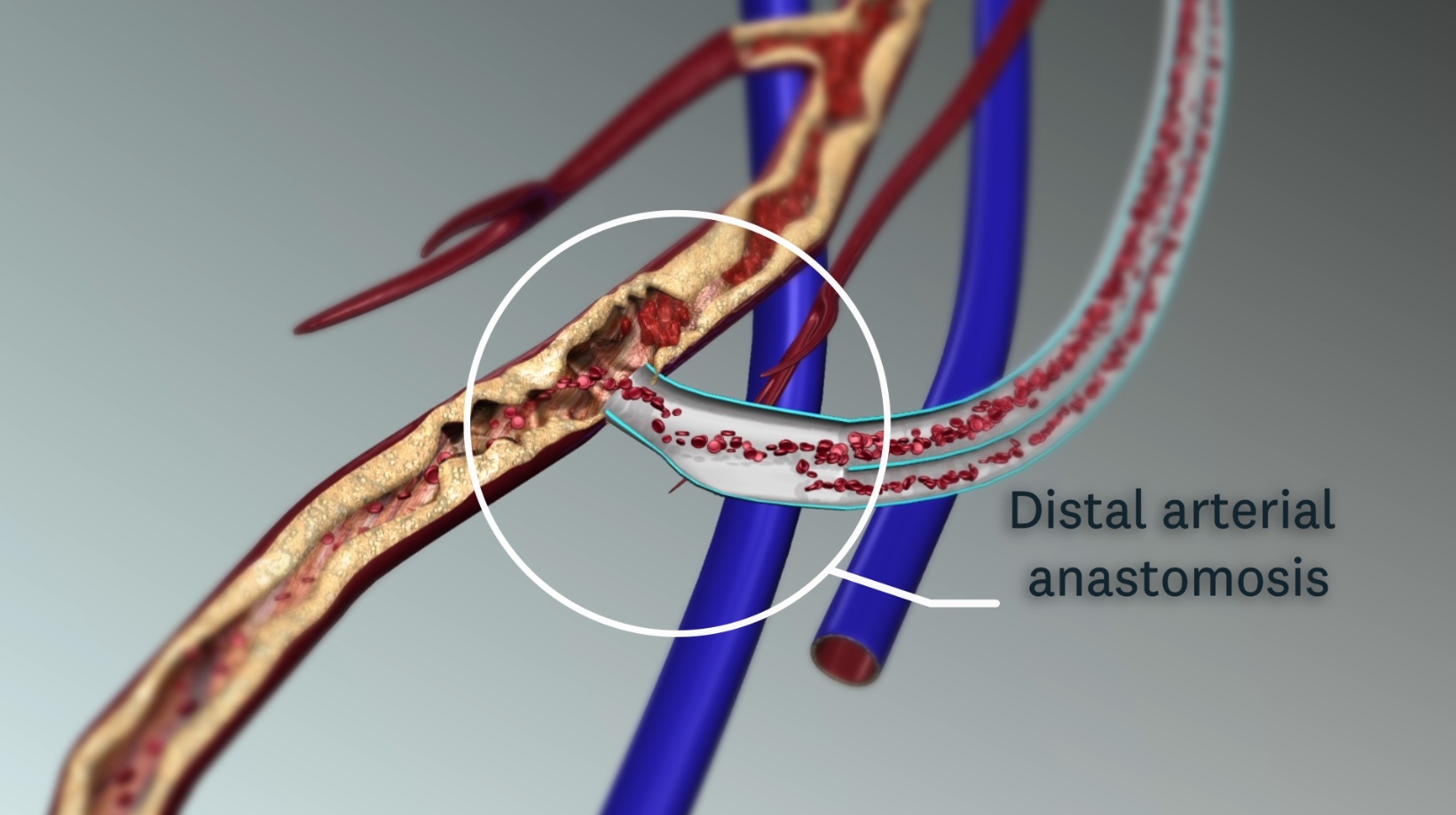
Reducing water-hammer trauma
Bench testing on a prototype showed minimal pressure loss along the distal graft segment and improved flow, and the added flow is intended to prevent the slow-flow thrombosis that occludes grafts in low-outflow limbs. Testing also pointed to a second effect: a reduction in the "water hammer" (blood hammer) effect at the distal anastomosis — the pressure shock that a pulsatile column of blood delivers against a poorly draining outflow. Softening that shock is intended to decrease trauma at the anastomosis in low-outflow states.
Whether these design effects translate into improved patency in patients is a question for preclinical and clinical evaluation. The device builds on the established DAVF concept with refinements intended to make it easier to place, gentler on the limb, and more durable in exactly the patients whose grafts are hardest to keep open.
Investigational status: Principal Medical's portfolio platforms and the products referenced here are currently in development and are not yet cleared or approved by the U.S. Food and Drug Administration.